
The Canadian health-care system is having difficulties: over-lengthy wait-times for elective surgeries, longer waits for specialist consultations, procedures, and some specialty treatments. Access to family doctors is reduced across the country.
Why is this? It’s important for all practitioners to think about these problems and consider the best approach to alleviate them.
Background to the current problems
The Barer-Stoddart Report of 1991
A frequent failing of governments of all stripes is to take decisions which, at the time seem to make sense, but turn out to be problematic over the years without rigorous follow-up. This report came out some 34 years ago when governments across Canada saw health care costs rising.
What to do? The Barer-Stoddart Report found a supposed cause and answer: health care economists Drs. Morris Barer (PhD) and Greg Stoddart (PhD) thought medical costs were largely driven by physicians and surgeons, and were rising because of the expensive activities of doctors.
Were there too many doctors? Fewer doctors would lead to fewer costs. Cut the number of trainees entering Canadian medical schools and voila! Problem solved. Fewer doctors would result in medical expenses lowering or plateauing. Medical school admissions were cut 10% and some schools were even paid to reduce the entry of medical students. This policy lasted some 10 years, and now seems crackpot. Although many of us saw it was likely a mistake at the time, governments (in this case the Mulroney government) and many administrators thought it a reasonable temporary approach.
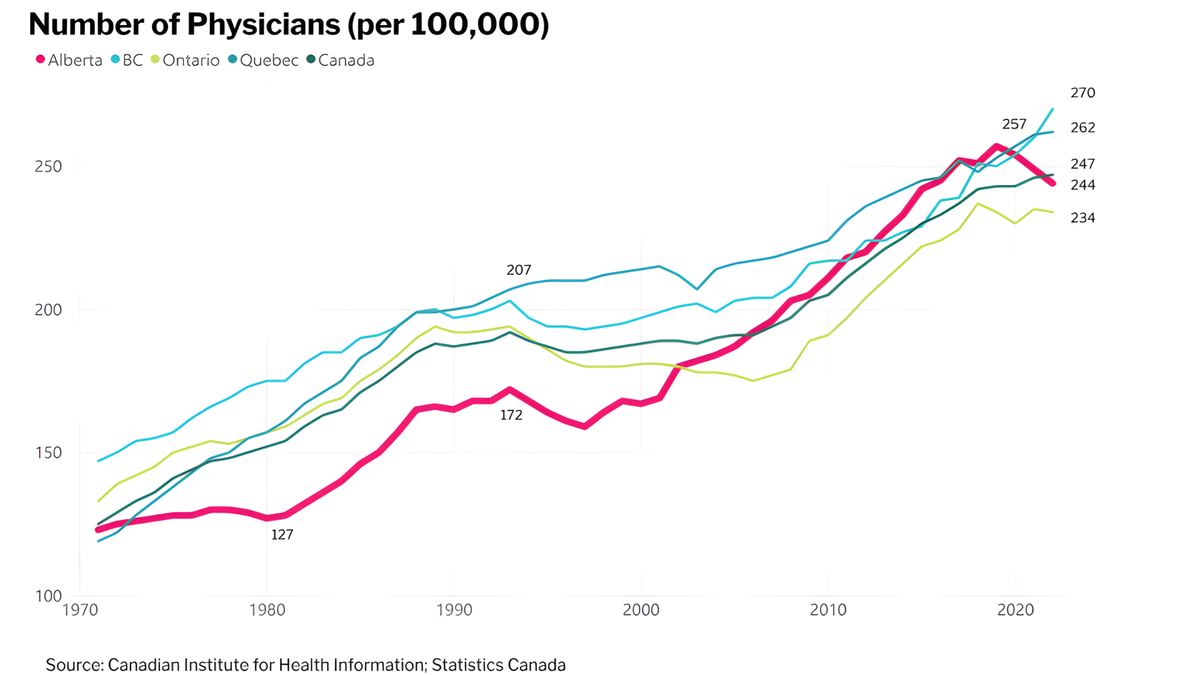
Barer and Stoddart did say (in small print) that the number of doctors should probably be based on the population at any one time… but governments forget. In the early 2000’s, the number of doctors started to increase in an attempt to match population increase, but at 2.4 doctors/100,000 population, we’re still well below the number of doctors in countries with dual practice systems (around 4 docs/100,000 capita) .
It's easy to point blame at a couple of economists for the difficulty we’re in, but we’re all partly to blame for not warning this would happen if the Canadian population was to greatly increase. Now we are seeing the downside of this “planning” with an acute shortage of medical staff, both of family physicians and other specialists – as well as nursing and top-class support staff.
Insufficient number of specialists and family doctors in training
This can be seen, as an example, in oncology. For years, Canada relied on importing specialist oncologists (e.g., radiation oncologists) to fill radiotherapy units across the country. This movement from overseas has slowed recently, but training positions in oncology remain unfilled to the level required for an aging population. And this is just one specialty having recruitment problems across the country. Family medicine, critically, is seeing many fewer trainees applying for residencies.
Increased population of Canada
The population of Canada has steadily increased since the time of the B-S report – over the last 34 years our population has increased by approximately 13.75 million people – almost a 33% rise. On population head counts alone we would need an increase of one-third as many doctors as in 1991. But this simple solution is insufficient, being further complicated by population aging.
Population aging
Together with the increase in Canada’s population, our population has aged. Statistics Canada data shows that the number of people aged 15-64 compared to those 65 and over, has dropped from 5.9 younger people to every older person in 1991, to 3.4 younger people to every older person in 2025. Older people use the health care system much more frequently than fitter younger people.
Increased complexity of therapies being delivered
Couple this with effective new therapies being used in an aging population, and you have increased demand for consultations and follow-up in order to deliver more complex therapies. More time is required to deal with side-effects, toxicities and other management issues such as explanations and answering questions after Dr. Google has been consulted. It’s easy to see why the nation’s ER departments are over-crowded with long delays before being seen by a clinician.
Bill-11 from Alberta’s United Conservative Party is an authorizing bill with first reading on November 24, 2025. It amends several health statutes, though doesn’t implement programs or set operating standards. This will occur in time through the Alberta Ministry of Health with consultation from Alberta Health Services, the Alberta Medical Association and College of Physicians & Surgeons of Alberta.
Bill-11 creates regulatory authority in several areas. Firstly, regulations authorizing which specialty clinicians may practice both publicly and privately. For example, at present, family doctors and specialist oncologists are not included in the plans. Secondly, it authorizes development of contracts stipulating time requirements for service within the public heath system, or procedure volume limits. Thirdly, it allows determination of geographic restrictions on dual practice. And fourthly, it will detail any penalties for non-compliance.
The Canada Health Act (CHA) sets out criteria that provincial health insurance plans must meet to receive federal funds. Medically necessary hospital, physician or surgical services must be insured by the provincial plan. Some health services such as prescription drugs and many mental health services, are not required by the CHA to be insured. Provinces can provide insurance for other health services beyond those described in the CHA. Hence, publicly insured health services vary across the country.
Possible pros of the dual system
- The hope is that higher total numbers of elective procedures, consultations and surgeries might be performed with the addition of after-hours private evening and weekend sessions rather than continuing with current hours in the public system alone (as long as staffing is available). But the evidence for this hope is sparse. These increased procedure numbers would especially affect orthopedics, ophthalmology and plastic surgery.
- While overall costs to the public will increase if they see a practitioner privately, costs to the public system, in theory, should remain similar unless too many private cases with complications are transferred to the public system.
- Patients in the public system might appreciate that they have a choice undertaking elective procedures either in the public or private system.
- Easier cases (those less likely to have complications) would tend to be done in the private system.
- Interruptions of service due to various professional associations withdrawing services may be less likely in a private system than in the public system.
- Private health insurance would become available. International companies (e.g. Aviva) would likely offer insurance in Canada.
- Private and public medicine work together best in large cities where shortages of specialist staffing is less of an issue. This may encourage recruitment of some specialists.
Possible cons of the dual system
- Emergency surgeries and consultations in hospitals could have difficulties finding required staff in a critical shortage specialty (such as anesthesia) if they are over-engaged in working in the private system but are also required for urgent work in the public system. Call schedules would have to be extremely carefully worked out, and private procedures cancelled if specialist physicians are unavailable.
- Serious surgical complications in the private system will likely be managed by transfer to the public system.
- There will be those being cared for in the public system who feel resentment that other members of society are receiving care because they’re able to afford private care. There would be the perception of queue jumping – although serious, difficult cases would continue to have priority in public hospitals.
- Harder cases which may have a higher likelihood of complications will tend to be done in the public system with its multiple specialist back-up.
- The possibility of abuse of the system by some specialists shirking the public system by spending less than their contracted time in the public system.
- Large multi-national health insurance companies may become a problem by increasing costs in the private system.
- Private practice is usually not feasible in smaller cities due to limited specialist staffing.
Some guardrails
- Cancer surgeries, radiation therapy and complex chemotherapy are best done by a team in the public system. Exceptions might be private delivery of standard chemotherapy in a stable patient who has access to a cancer centre and oncologist if problems occur.
- Anyone working in the private system should have a formal contract determining hours of service which would be enforced.
- The heads of medical departments in public hospitals and the registrar of the College of Physicians & Surgeons of Alberta should have full access to review all activities of private clinics.
- Any doctor participating in private surgeries, procedures or consultations should be a member of staff of a public hospital department and have admitting privileges at a public hospital.
- Regular reviews of staffing levels and numerical data with outcomes is needed.
- The idea of extra-billing in the public system – outlawed by the Mulroney government – should be laid to rest.
My experience with the private system in the UK
I worked in the U.K.’s National Health Service for six years before coming to Canada. One year was spent in hospitals in general surgery and medicine around Edinburgh. No staff surgeon or physician had a private practice.
I spent another year in a general hospital in the London area and then four years at St. Bartholomew’s Hospital and the Royal Marsden Hospital studying oncology. There was private practice at all hospitals. At the Royal Marsden, this involved the surgeons but also one or two radiation specialists and one medical oncologist. The non-surgical private practitioners’ work involved special counselling sessions and in-depth explanations of treatment planning. I never saw any therapeutic advantage being given to private patients. The surgical, radiation and medical oncological consults occurred in private facilities, although actual radiation and medical therapies were delivered at the Royal Marsden.
I occasionally participated in general medical locums in Harley Street where private patients were surprised to see a young doctor covering for an ill private physician. Occasionally the consultations were odd. I recall seeing a well-known author’s son who was allergic to heather when he participated in shooting grouse in the borders of Scotland. A special “heather mixture” was in the refrigerator for the poor lad to administer subcutaneously!
My overall feeling about Harley Street was that it was a great place if there’s nothing very much wrong with you – plush waiting room, up-to-date magazines and polite doctors. The other thing I noticed were members of the UK government cabinet frequently using Harley Street!
I never saw anything that implied superior treatment was being given compared to the National Health Service. If anything, it was the other way around – at least as far as oncology was concerned. The therapies and managements available were much superior at the Royal Marsden to anywhere on the street. I often questioned patients as to why they weren’t participating in the activities of the publicly funded Royal Marsden.
The situation at present in Canada:
Access to private care has always been available in Canada for those wealthy enough and willing and able to travel out of country. Private radiology and plastic surgery have already been available for several years in Canada.
There is variation in practice rules across the country bordering in some cases on silliness. For example, in Quebec, it’s fine for some clinicians to run a weekend private practice by resigning from the public system on Friday afternoon, and applying to rejoin the public system on the following Monday. It is possible to fly to another province as a visitor and have a hip replacement or other surgery done privately which is not allowed to the local population.
I came to work in Canada in 1975 at the Cross Cancer Institute in Edmonton. The Canadian system has worked well for many years with most patients being seen reasonably quickly, having procedures performed promptly, and therapy instituted in a timely fashion. This is no longer the case. This seemed to become critically obvious during the pandemic when many experienced medical and nursing staff decided to retire, and the effects of the increased and aging Canadian population steadily took a grip. Also taking retirements were experienced receptionists who knew how to handle complex calls which now are often passed on to busy medical and nursing staff which interrupts their other duties.
Aggressive recruitment of specialist staff (e.g. anesthetists) and increasing specialist and general practitioner training positions may improve things over the next 10 years, but there is certainly no easy or rapid solution. Great care will have to be taken to ensure no worsening of the situation if the dual path goes ahead. At best, the dual path might encourage some experienced specialists to move to Alberta.
Author's post-script: I’d like to thank those who reviewed this article and suggested modifications and additions. These included: Dr. Martin Atkinson, Dr. Paul Armstrong, Dr. Eldon Shaffer and Dr. Jon Meddings.
Editor’s note: The views, perspectives and opinions in this article are solely the author’s and do not necessarily represent those of the AMA.
Banner image credit: Gerd Altmann, Pixabay.com